Esophageal Tracheal Combitube
When rescue breathing is needed, such as during CPR, the rapid establishment and maintenance of a clear airway is a primary priority. Bag-valve-mask ventilation has significant drawbacks, such as the risk for aspiration of gastric contents, and ideally should only be used for short periods of time. Tracheal intubation is preferred for rescue breathing but requires a skilled provider, proper positioning of the patient and provider, and other provisions that are not always immediately available.
In 1981 at the Medical University of Vienna, Drs. Michael Frass and Jonas Zahler began to design an emergency airway. They wanted one that could be inserted quickly and easily, without a laryngoscope, and that could also function whether it was placed in the esophagus or, unintentionally, in the trachea. After Dr. Reinhard Frenzer joined them in 1983, they completed the design and prototype for the esophageal tracheal combitube (ETC). Commercial production of the Combitube began in 1988.
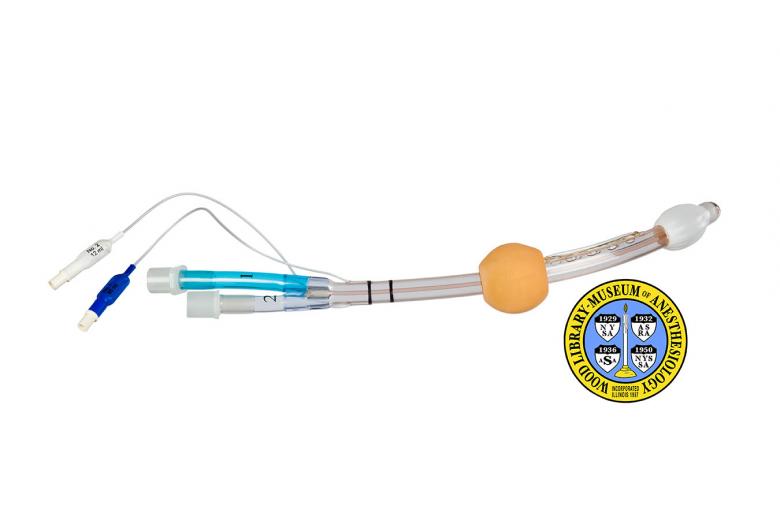
It is two tubes (or lumens) in one. When placed into the esophagus, the longer, blue colored tube (the esophageal lumen), is used. To seal and anchor the tube, a large cuff or balloon is inflated in the pharynx after insertion. A cuff at the distal end of the tube and perforations in the lumen, between the two cuffs, allow for the ventilation of the patient. If it is placed in the trachea the shorter, clear tube (the tracheal lumen) is used. Like an endotracheal tube, the tracheal lumen is open at the distal end.
Catalog Record: Esophageal Tracheal Combitube
Access Key: akgv
Accession No.: 2005-05-20-1 A
Title: [Esophageal tracheal combitube / Michael Frass, Reinhard Frenzer, and Jonas Zahler.]
Author: Frass, Michael.
Author: Frenzer, Reinhard.
Author: Zahler, Jonas.
Title variation: Alt Title
Title: Combitube : esophageal tracheal airway.
Title variation: Alt Title
Title: Combitube regular.
Title variation: Alt Title
Title: ETC.
Publisher: [Argyle, New York?] : [Sheridan Catheter Corporation?], [1986-1988].
Physical Descript 1 esophageal tracheal airway : plastics, rubber ; 8 x 37.5 x 3 cm.
Subject: Airways.
Subject: Airway Management Equipment.
Subject: Respiration, Artificial – instrumentation.
Subject: Esophageal Airway Devices.
Subject: Intubation, Intratracheal – instrumentation.
Subject: Cardiopulmonary Resuscitation – instrumentation.
Note Type: General
Notes: The year 1986 was chosen for the earliest year that this ETC could have been
made, and 1988 as the latest due to the following reasons: Dr. Frass, who
donated this airway to the WLM, referred to it as a prototype. The American
company, Sheridan Catheter Corporation began to manufacture the Esophageal
Tracheal Combitube (ETC) in 1988. The three inventors encountered
difficulties in finding a manufacturer. The English abbreviation for ‘number’
(No.) is marked on the tube. The date range could change if documentation
indicates the range should be corrected.
Note Type: Citation
Notes: Title based on the first publications about the airway in 1987.
Note Type: With
Notes: The Esophageal Tracheal Combitube was donated with a 100 ml plastic syringe
for inflation of the airway’s two cuffs.
Note Type: Citation
Notes: Frass M, Frenzer R, Ilias W, Lackner F, Hoflehner G, Losert U. The esophageal
tracheal Combitube (ETC): animal experiment results with a new emergency tube
[German]. Anasth Intensivther Notfallmed. 1987;22(3):142-144.
Note Type: Citation
Notes: Frass M, Frenzer R, Zahlet J. Respiratory tube or airway. US patent 4,688,568
August 25, 1987.
Note Type: Citation
Notes: Frass M, Frenzer R, Zdrahal F, et al. The esophageal tracheal combitube:
preliminary results with a new airway for CPR. Ann Emerg Med. 1987
Jul;16(7):768-772.
Note Type: Citation
Notes: Michael TA, Lambert EH, Mehran A. “Mouth-to-lung airway” for cardiac
resuscitation. Lancet. 1968;2(7582):1329.
Note Type: Citation
Notes: Oczenski W, Krenn H, Dahaba AA, et al. Complications following the use of the
Combitube, tracheal tube and laryngeal mask airway. Anaesthesia.
1999;54(12):1161-1165.
Note Type: Citation
Notes: Rich JM, Mason AM, Bey TA, Krafft P, Frass M. The critical airway, rescue
ventilation, and the Combitube: part 1. AANA J. 2004;72(1):17-27.
Note Type: Citation
Notes: Schofferman J, Oill P, Lewis AJ. The esophageal obturator airway. A clinical
evaluation. Chest. 1976 Jan;69(1):67-71.
Note Type: Physical Description
Notes: One long airway with two proximal lumens, and two filling ports for two
cuffs; The airway measures approximately 37.5 cm in length when measured end
to end in a straight line; When measured against the curve at the distal end,
the length is approximately 40 cm; On the end opposite the two lumens is a
cuff, referred to as the tracheoesophageal cuff or the distal cuff; Moving
from the tracheoesophageal cuff (TEC) toward the other end of the airway, a
second cuff is located approximately 9 cm from the TEC; This second cuff is
referred to as the pharyngeal balloon, or pharyngeal cuff; Between these two
cuffs eight perforations in the pharyngeal (or esophageal) lumen;
Approximately 7 cm from the pharyngeal balloon two black rings are marked on
the airway; Located about 2.5 cm beyond the rings are two inflation ports
with approximately 16.5 cm of thin tubing connecting each to the airway; One
of the ports is blue and marked with the following text, “NO. 1 [new line]
100 ml”; The other port is white and marked with, “No. 2 [new line] 15 ml”;
The lumen used for ventilation when the airway is placed in the esophagus
(the pharyngeal or esophageal lumen) is blue, marked with, “No. 1”, and
measures approximately 2 cm longer than the tracheal lumen: The lumen used to
ventilation the patient if the airway is placed in the trachea (the
tracheoesophageal or tracheal lumen) is clear and marked with, “No. 2”.
Note Type: Reproduction
Notes: Photographed by Mr. Steve Donisch on January 14, 2013.
Note Type: Acquisition
Notes: Donated to the WLM by one of the inventors, Michael Frass, MD
Note Type: Historical
Notes: When rescue breathing is needed, such as during CPR, the rapid establishment
and maintenance of a clear airway is a primary priority. Bag-valve-mask
ventilation has significant drawbacks, such as the risk for aspiration of
gastric contents, and ideally should only be used for short periods of time.
Tracheal intubation is preferred for rescue breathing but requires a skilled
provider, proper positioning of both the patient and provider, and other
provisions that are not always immediately available. In November of 1981 at
the Medical University of Vienna, when Dr. Michael Frass was beginning a
residency in internal medicine and Jonas Zahler was a staff physician, they
began to think about how the esophageal obturator airway (EOA) might be
redesigned to overcome some of its disadvantages. At this time the EOA
(introduced in 1968 and developed by Drs. T.A. Don Michael, E.H. Lambert, and
A. Mehran) was the only option between bag-valve-mask ventilation and the
insertion of a tracheal tube. Since its introduction, a number of
shortcomings had come to light, including difficulties in maintaining the
seal of the EOA’s face mask, especially during transport, and occurrences of
unrecognized placement of the EOA in the trachea rather than the esophagus.
Although this latter complication occurred infrequently it had resulted in
patient deaths.
Note Type: Historical
Notes: Drs. Frass and Zahler not only wanted an airway that could be inserted
quickly and easily, without a laryngoscope, but one that could function
whether it was placed in the esophagus or, unintentionally, in the trachea.
After Dr. Reinhard Frenzer joined Drs. Frass and Zahler in 1983, they
completed the design and prototype for what they referred to as an esophageal
tracheal combitube (ETC). They experienced some difficulties with the patent
application process and in finding a manufacturer interested in producing
their invention, but in 1987 the U.S. application was granted and they
reached an agreement with The Sheridan Catheter Corporation, of Aargyle, New
York. The commercial production of ETCs began in 1988. During the 1990s,
Kendall International acquired Sheridan Catheter Corp., and Tyco
International acquired Kendall.
Note Type: Historical
Notes: Also referred to as the Combitube, it is two tubes in one. If the tube is
placed into the esophagus (as is what occurs with most blind insertions) the
longer, blue colored lumen, called the esophageal lumen, is used to ventilate
the patient. To seal and anchor the tube, a large cuff or balloon is inflated
in the pharynx after insertion. The esophageal lumen is closed at the distal
end. A cuff at the distal end of the tube and perforations in the esophageal
lumen, between the two cuffs, allow for the ventilation of the patient when
the tube is placed in the esophagus. If the ETC is placed in the trachea the
shorter, clear lumen, called the tracheal lumen, is used. Like an
endotracheal tube, the tracheal lumen is open at the distal end.
Note Type: Historical
Notes: Interestingly, the esophageal tracheal combitube (ETC) shares two notable
dates with another significant airway, the laryngeal mask airway (LMA): In
1981, the year in which Drs. Frass and Zahler first thought about their new
airway, Dr. Archie I.J. Brain began to develop the LMA. Both airways became
commercially available in Great Britain in 1988.
Note Type: Publication
Notes: Frass M. Development, patent procedure, and 15 years experience: Combitube –
from bench to bedside. Curr Opin Clin Exp Res 2:31-38, 2000.
Note Type: Publication
Notes: Heinz WC, Sheridan DS. Inventor: The Dave Sheridan Story. Albany, N.Y.:
Albany Medical Center; 1988.
Note Type: Exhibition
Notes: Chosen for the WLM website (noted April 2, 2013).
