Semoff Vital Capacity Apparatus
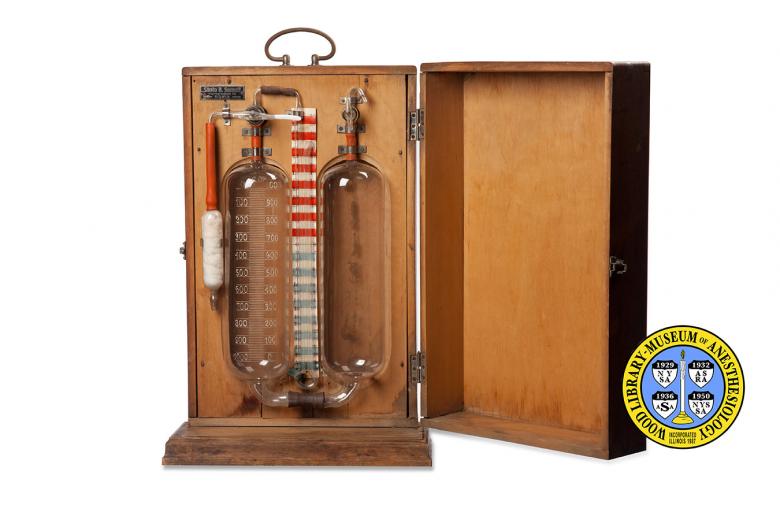
Built-into a wooden carrying case, this portable apparatus for measuring vital capacity was made in Sofia, Bulgaria by Santo B. Semoff. Vital capacity is one of the most basic measurements of lung function. It is the amount or volume of air a person can exhale after taking the deepest breath he can. The term was coined by British surgeon John Hutchinson around 1846. Hutchinson noted that vital capacity is related to, among other things, height: the taller you are the larger your vital capacity. A person’s vital capacity can be reduced by a wide variety of diseases, including heart failure, fibrosis of the lungs, and neuromuscular disorders such as myasthenia gravis. Vital capacity is usually measured during “spirometry,” a group of breathing tests that measure how much and how quickly you can move air out of your lungs.
When anesthesiologists first meet and assess their patients before surgery, lung function is one of the things they evaluate. Most patients do not need breathing tests for this, as a health history and physical exam are often enough to detect any potential problem. Anesthesiologists will look for spirometry results in people with certain diseases, symptoms, or health histories. In these cases, the results provide anesthesiologists with important information, such as indications that a patient may need breathing assistance after surgery.
Catalog Record: Semoff Vital Capacity Apparatus
Access Key: akhu
Accession No.: 2004-03-27-1
Title: Semoff [vital capacity apparatus].
Corporate Author: Santo B. Semoff.
Publisher: Sofia : Santo B. Semoff, [1880-1935].
Physical Descript: 1 scientific device ; glass, metals, rubber, wood : 49 x 32.5 x 15 cm.
Subject: Vital Capacity – instrumentation.
Subject: Lung Volume Measurements – instrumentation.
Note Type: General
Notes: Title determined by the WLM Museum Registrar and the WLM Curator’s
identification of the object; The early year in the date range for possible
year of manufacture is base on the Romanization of the text in the makers
plate (after Ottoman empire?). The later date is based on age of equipment
and the volume of scientific activity on pulmonary function. The date range
could change if documentation indicates the range should be corrected.
Note Type: Citation
Notes: Eisenkraft JB, Cohen E, Neustein SM. Anesthesia for thoracic surgery. In:
Barash PG, Cullen BF, Stoelting RK, Cahalan MK, Stock MC, Ortega R, eds.
Clinical Anesthesia. 7th ed. Philadelphia: Wolters Kluwer Lippincott Williams
& Wilkins; 2013:1030-1034.
Note Type: Citation
Notes: Petty TL. John Hutchinson’s mysterious machine. Trans Am Clin Climatol Assoc.
1987;98:11–20.
Note Type: Citation
Notes: Singh-Radcliff N. Flow volume loops. In: The 5-Minutes Anesthesia Consult.
Philadelphia: Wolters Kluwer Lippincott Williams & Wilkins; 2013:400-401.
Note Type: Physical Description
Notes: A wooden case that opens in the front, with two metal hinges and one latch; A
system of specially made glass laboratory held together with rubber tubes and
held in place with metal clamps; The two largest pieces are glass tubes of
the same size, approximately 27 cm in height and 7.5 cm in diameter; Each
tube is rounded at the ends and tapered into small port like openings on both
the top and bottom; The large glass tube on the left has two graduation
scales marked in “C.C.”; The graduation on the left starts in 0 at the top
and ends in 1000 at the bottom; The scale on the right is the opposite,
starting with 1000 at the top and 0 at the bottom; Inside the bottom of the
large tube on the right is a small amount of dried residue, which is a very
light reddish brown in color; Between these two large tubes is another scale,
printed on thick paper, that runs vertically with 0 at the center; From the
center or 0 to the top of the paper scale the graduation is marked in even
numbers from 0 to 32; The graduation marks are created by alternating 1 cm
stripes of red and white; From the center to the bottom of the paper scale
the graduation is marked in even numbers from 0 to 32, and the graduation
marks are created by alternating 1 cm stripes of blue and white; All of the
other glass pieces are difficult to describe, but noteworthy is a smaller
glass tube to the left of the graduated large glass tube; This smaller glass
tube is approximately 9.5 cm in length and 2.5 cm in diameter; Like the
larger tubes, this one is rounded at the ends, which tapered into small
openings; This smaller tube is stuffed with wool, cotton, or possibly
asbestos, and the glass at the lower end is darkened as if it has been
exposed to high temperatures in the past; A metal plate with the makers
identification and address is nailed to the inside, as well as outside, of
the box; Text on the plate includes, “Santo B. Semoff,” new line,
“Karnigradska 13.”, new line, “SOFIA”; Pieces of the system have come loose
(two rubber bulbs, rubber tubing, and what might be a glass plug), and are
stored in a small box next to the object.
Note Type: Reproduction
Notes: Photographed by Mr. Steve Donisch on January 15, 2013.
Note Type: Historical
Notes: The object described in this record has been identified as likely to be an
apparatus for measuring vital capacity. Contained within a wooden case this
portable device was made in Sofia, Bulgaria by Santo B. Semoff. Vital
capacity is one of the most basic measurements of lung function. It is the
amount or volume of air a person can exhale after taking the deepest breath
he can. The term was coined by British surgeon John Hutchinson around 1846.
Hutchinson noted that vital capacity is related to, among other things,
height: the taller you are the larger your vital capacity. A person’s vital
capacity can be reduced by a wide variety of diseases, including heart
failure, fibrosis of the lungs, and neuromuscular disorders such as
myasthenia gravis. Vital capacity is usually measured during “spirometry,” a
group of breathing tests that measure how much and how quickly you can move
air out of your lungs.
When anesthesiologists first meet and assess patients before surgery, lung
function is one of the things they evaluate. Most patients do not need
breathing tests for this, as a health history and physical exam are often
enough to detect any potential problem. Anesthesiologists will look for
spirometry results in people with certain diseases, symptoms or health
histories. In these cases, the results provide anesthesiologists with
important information, such as indications that a patient may need breathing
assistance after surgery.
Note Type: Publication
Notes: Derenne JP, Zelter M. Who first described clinical spirometry [in French]?
Rev Mal Respir. 2002;19(3):385-386.
Note Type: Publication
Notes: Petty TL. John Hutchinson’s mysterious machine revisited. Chest. 2002;121(5
suppl):219S-223S.
Note Type: Exhibition
Notes: Chosen for the WLM website (noted June 10, 2013).
